 Tasselline | Latest Articles By Singaporeans, for Singaporeans Article Site for Singaporeans
Tasselline | Latest Articles By Singaporeans, for Singaporeans Article Site for Singaporeans
M almost freaked out when she saw a patch of fresh blood staining her panty in the morning. She had had sexual intercourse with her husband the night before. She woke him up straightaway and rushed to my clinic. M, 28, a first-time mum, was in her 12 weeks of pregnancy. She related the incident with some embarrassment. “Doc, will I have miscarriage?” she asked.
Ultrasound examination revealed that the baby was active with a normal heart rate of 150 beats per minute. The placenta was at the normal site with no sign of detachment. Vaginal examination showed that she had a 1cm polyp protruding from the cervix (the neck of the womb), with a small amount of blood on its surface. I reassured M that there was no cause for alarm and that I would watch the bleeding closely.
M was happy to find that the spotting stopped 2 days later. Her pregnancy progressed normally albeit with an increase in yellowish vaginal discharge. At around 21 weeks of pregnancy, the discharge turned pinkish with a slight smelly odour. Her cervical polyp had bled again. I advised her to have it removed and this was done under sedation the next day. Microscopic examination of the polyp revealed that it was non-cancerous.
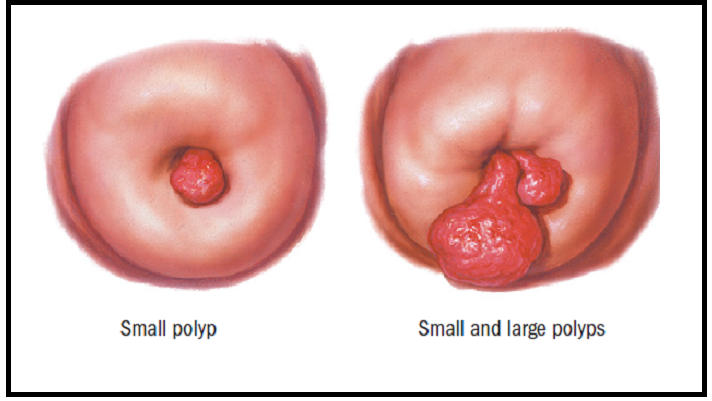
Cervical polyps are growths that appear like bulbs on thin stems on the cervix (fig 1). They are usually cherry-red to reddish-purple in appearance but may appear greyish-white. They are usually small, varying in size from 1 cm to 2cm, and can occur alone or in groups.
The cause of cervical polyps is not well understood, but they are associated with chronic inflammation of the cervix or local congestion of cervical blood vessels. They may also result from an abnormal response to the female hormone, oestrogen.
They are usually non-cancerous. Very rarely (less than 2%), cancerous lesions may present as polyps and thus it is recommended that all symptomatic polyps should be removed and examined for signs of cancer.
Cervical polyps can be found in women at any stage of pregnancy. Most of the time, patients have symptoms of vaginal bleeding, bleeding after sexual intercourse or vaginal discharge. Occasionally, the polys do not have any symptoms and are only discovered during vaginal examination. It is difficult to establish whether the polyp is a pre-existing condition or one that has developed during pregnancy.
Bleeding in pregnancy from a cervical polyp poses a quandary to the mother. Can the polyp cause miscarriage or premature birth? Can it be cancerous? Would the procedure of its removal have a negative impact on the pregnancy?
Currently, if the polyp is asymptomatic, conservative management is preferred. If symptoms are present, the polyp should be removed as infection may set in and premature birth may result.
Removal of cervical polyps can be done under sedation with antibiotic cover. The polyp should preferably be assessed with a colposcope to ascertain its appearance, location, form and length. It is then removed by a polyp forceps. The risk of miscarriage is minimal. M recovered from the polyp removal satisfactorily other than a slight vaginal bleeding for a few days. Her pregnancy progressed well. She is now awaiting delivery in a week’s time.
Want to arrange for an appointment with Dr Peter Chew – an experienced gynaecologist based in Gleneagles Medical Centre? Contact us via email or phone here. Read up on our next article on Pregnancy & Diabetes here.